
A Quick Guide to Respiratory Sensitization Testing
Regulatory Challenges, Mechanistic Understanding, and the Emerging Role of NAMs

Introduction
For toxicologists and regulatory professionals, protecting workers from occupational asthma and airway hypersensitivity is a top-tier priority. Yet, respiratory sensitization remains one of the most complex and unresolved endpoints in industrial toxicology.
Historically, this endpoint has lacked standardized, predictive testing frameworks, making hazard identification highly reliant on retrospective human data. Today, however, the landscape is evolving. Advances in Adverse Outcome Pathways (AOPs) and New Approach Methodologies (NAMs) are enabling a shift toward mechanistically informed, non-animal testing strategies.
This guide provides a structured overview of the biological mechanisms, testing landscape, and regulatory expectations for respiratory sensitization, tailored for industry professionals navigating chemical safety and product development. While this guide provides a broad overview of the endpoint and current regulatory practices, particular attention is given to how emerging non animal methodologies are helping to address key gaps in the field.
Key takeaways
- Respiratory sensitization is a scientifically evolving and regulatorily challenging endpoint with significant implications for occupational and public health.
- Respiratory sensitization assessment is gradually transitioning from reliance on imperfect surrogate methods toward a more predictive, mechanism-driven discipline.
- Among the emerging non-animal approaches, GARD®air represents one of the most well-characterized and commercially available assays.
Author: Andy Forreryd, PhD
In vitro toxicology expert, member of the OECD expert group on respiratory sensitization, and ISO/TC 194/WG 8 on irritation and sensitization.
Definition: Respiratory Sensitizers and Sensitization
A respiratory sensitizer is a substance that induces immune-mediated hypersensitivity of the respiratory tract, resulting in allergic reactions upon re-exposure.
Respiratory sensitization is a systemic immunological process that can lead to long-term or irreversible effects. The most well-recognized adverse outcome is occupational asthma (OA), although other clinical manifestations, such as rhinitis, conjunctivitis, and rhino-conjunctivitis, may also occur.
Classes of sensitizers
Respiratory sensitizers are broadly divided into two categories:
- Low Molecular Weight (LMW) sensitizers (< 1000 Da): Small reactive chemicals that act as haptens and require covalent binding to endogenous proteins to become immunogenic (e.g., isocyanates, acid anhydrides, reactive dyes).
- High Molecular Weight (HMW) sensitizers (> 1000 Da): Typically proteins that are inherently immunogenic (e.g., enzymes, flour dust, natural latex).
Two-phase immunological mechanism
Respiratory sensitization develops through two distinct phases: an induction phase, during which sensitization is established, and an elicitation phase, during which clinical symptoms occur upon re-exposure.
Induction phase
- Occurs without clinical symptoms.
- Triggered by inhalation or dermal exposure.
- Leads to immune activation and development of immunological memory.
Elicitation phase
- Occurs upon re-exposure.
- Even trace levels can trigger a reaction.
- Results in respiratory hypersensitivity, including bronchoconstriction and asthma.
Why Is Testing Important?
Respiratory sensitization represents a major occupational health hazard, contributing significantly to adult-onset asthma. Once sensitization has occurred, individuals may react to extremely low exposure levels, and symptoms may persist even after exposure ceases.
Early identification is critical because:
- Sensitization can develop after repeated low-level exposure.
- No safe exposure threshold can be reliably defined.
- The condition is often irreversible.
- Occupational exposure limits (OELs) may not prevent elicitation.
From a regulatory and industrial perspective, testing supports:
- Hazard classification and labelling.
- Worker protection and exposure control strategies.
- Safer product design and substitution decisions.
However, both the diagnosis and prospective prediction of respiratory sensitization is inherently difficult due to:
- Lack of specific biomarkers.
- Difficulty distinguishing sensitization vs irritation.
- Limited availability of reliable human data.
Regulatory landscape
Respiratory sensitization is globally recognized as a critical hazard endpoint. However, regulatory approaches remain non-harmonized, data-limited, and heavily dependent on expert judgement. (Reference: OECD Detailed Review Paper, 2025 )
Global framework: UN GHS
Under the United Nations Globally Harmonized System (GHS):
- Respiratory sensitization is defined as hypersensitivity of the airways following inhalation exposure.
- Classification is primarily based on human evidence.
- A weight-of-evidence (WoE) approach integrates human, animal, and mechanistic data
- Proof of an immunological mechanism is not required.
A key limitation is that the respiratory sensitization provisions within GHS have not evolved to incorporate modern NAMs to the same extent as skin sensitization frameworks.
European Union: REACH, CLP, PPP, BPR
The EU regulatory framework for chemical safety is built on four interconnected regulations:
- REACH (EC 1907/2006) – general chemical safety and registration.
- CLP (EC 1272/2008) – classification, labelling, and packaging.
- PPP (EC 1107/2009) – plant protection products.
- BPR (EU 528/2012) – biocidal products.
Together, these define both data requirements and hazard communication in the EU.
Classification under CLP
- Classified as Resp. Sens. 1 (H334).
- May trigger Substances of Very High Concern (SVHCs) designation under REACH Article 57(f).
- Classification triggers strict hazard communication and risk management requirements.
Regulatory assessment and data requirement
- Respiratory sensitization is not a standard data requirement under REACH.
- The European Chemicals Agency (ECHA) provides guidance incorporating AOP concepts and available methods, but currently does not recommend generating new data using non-validated assays.
- No validated in vivo or in vitro methods are available; therefore, current assessment relies on WoE approaches using existing data.
- Skin sensitization data are frequently used as supporting information, but cannot exclude respiratory sensitization risk.
Ongoing regulatory developments
- The Partnership for the Assessment of Risks from Chemicals (PARC) initiative is actively developing next-generation, NAM-based approaches for respiratory sensitization.
- In 2026, the European Commission presented a roadmap to replace animal models with alternative methods for sensitization endpoints by 2029.
United States: TSCA, FIFRA (EPA) and Occupational Safety (OSHA)
The U.S. regulatory landscape for respiratory sensitization combines federal legislation with agency-driven risk assessment and occupational safety frameworks:
- TSCA (Toxic Substances Control Act) – industrial chemicals (EPA, Office of Pollution Prevention and Toxics).
- FIFRA (Federal Insecticide, Fungicide, and Rodenticide Act) – pesticides (EPA, Office of Pesticide Programs).
- OSHA (Occupational Safety and Health Administration) – workplace exposure and worker protection.
Together, these frameworks define risk evaluation, hazard identification, and occupational safety requirements in the U.S.
OSHA (workplace protection)
- Focuses on worker health protection and exposure control.
- Uses epidemiological, clinical, and mechanistic data within a WoE framework.
- Recognizes that both dermal and inhalation exposure contribute to sensitization risk.
EPA (TSCA / FIFRA)
- Evaluates respiratory sensitization for industrial chemicals and pesticides
- Relies heavily on:
- QSAR and structural alerts.
- Read-across approaches.
- Integrated WoE assessments.
- For HMW proteins, sensitization is often assumed by default.
- For LMW chemicals, assessment is case-by-case and data-limited.
Regulatory assessment and data requirement
- No standardized data requirements for respiratory sensitization testing under TSCA or FIFRA.
- Limited availability of human data for new chemicals, especially pre-market.
- Similar to the EU, no validated, widely accepted test methods are available.
- Regulatory decisions rely heavily on expert judgement and multiple indirect evidence streams.
Ongoing regulatory developments
- Strong regulatory and legislative emphasis on reducing animal testing and increasing use of alternatives.
- The EPA actively supports development of NAMs, Integrated Approaches to Testing and Assessment (IATA), and future Defined Approaches (DA).
- Collaborative initiatives (e.g., NIEHS / ICCVAM) are advancing respiratory sensitization NAMs, including the GARDair method.
- EPA programs are increasingly incorporating NAM data into WoE evaluations, although not yet as standalone decision tools.
Key regulatory takeaway
Across regions and sectors:
- Weight-of-evidence is the default approach.
- Validated predictive methods are lacking.
- Human data remain central to classification.
- There is a growing shift toward mechanistic, NAM-based strategies.
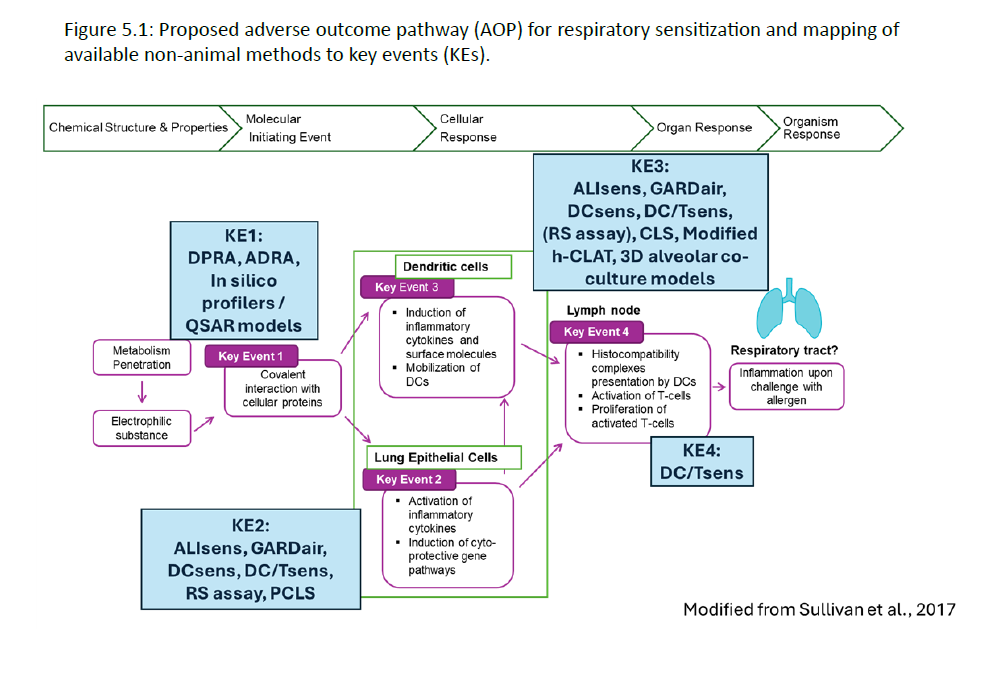
The Adverse Outcome Pathway (AOP) of respiratory sensitization
The Adverse Outcome Pathway (AOP) framework organizes mechanistic knowledge linking chemical exposure to respiratory hypersensitivity.
Building on established skin sensitization models, a draft AOP (AOP 39) has been proposed for LMW chemical respiratory sensitizers, but remains incomplete and under development (OECD Detailed Review Paper, 2025).
Core mechanistic sequence
The current understanding of respiratory sensitization can be described through the following key events (KEs):
Molecular Initiating Event/Key Event 1 (MIE/KE1): Protein binding (haptenation)
- Electrophilic chemicals bind to amino acid residues (e.g., lysine, cysteine) on skin or lung proteins, forming hapten-protein complexes
Key Event 2 (KE2): Epithelial cell signalling and activation
- Release of danger signals (alarmins) such as TSLP, IL‑25, and IL‑33, along with inflammatory mediators.
- Possible epithelial barrier disruption, increasing allergen penetration
Key Event 3 (KE3): Dendritic cell activation and maturation
- Uptake of hapten–protein complexes
- Upregulation of co-stimulatory molecules (e.g., CD80, CD86, CD54)
- Migration to lymph nodes
Key Event 4 (KE4): T-cell activation, proliferation, and polarization
- Activation of naïve CD4⁺ T cells
- Predominant skewing toward a Th2 phenotype (IL‑4, IL‑5, IL‑13)
- Additional involvement of Th17 and other immune pathways
Adverse Outcome (AO): Manifestation of respiratory hypersensitivity
- Immune memory: activation of adaptive immunity, potentially including IgE production
- Upon re-exposure: allergic respiratory hypersensitivity, including occupational asthma
Key scientific considerations
- The draft AOP is primarily applicable to LMW electrophilic chemicals.
- Not all sensitizers follow the same mechanism (e.g., metals).
- The pathway is not fully linear or universal, with multiple parallel immune processes.
- Sensitization may occur via both inhalation and dermal exposure.
- The site of exposure and the site of adverse outcome are not always identical.
Overall, the respiratory sensitization AOP remains less mature than that for skin sensitization, limiting its direct regulatory use.
Against this background, significant research efforts are focused on developing NAM-based approaches that target specific mechanistic events within the AOP and support more predictive, human-relevant hazard assessment.
Overview of available testing methods
Respiratory and skin sensitization share several mechanistic features, particularly during the early stages of the AOP. As a result, methods originally developed for skin sensitization can provide valuable mechanistic information relevant to respiratory sensitization.
However, important differences in target tissues, immune responses, and exposure routes mean that these methods cannot be directly extrapolated to respiratory sensitization without further adaptation and validation. Historically, respiratory sensitization has therefore remained a particularly difficult endpoint to assess, and researchers have relied on methods originally developed for either skin sensitization or inhalation toxicity studies, both in vivo and in vitro.
Despite decades of research, no testing method has yet achieved broad regulatory acceptance for the prediction of respiratory sensitizers. The current testing landscape reflects both the scientific complexity of the endpoint and the lack of fully established testing strategies. These challenges are not specific to any individual assay or technology, but instead arise from fundamental biological and regulatory limitations associated with respiratory sensitization itself.
Historically, considerable effort was devoted to the development of animal-based approaches. However, increasing ethical, regulatory, and scientific pressure to reduce animal testing has accelerated the search for alternative approaches. As a result, research and method development are now increasingly focused on NAMs, particularly those designed around mechanistic understanding of the respiratory sensitization AOP.
Animal-based approaches (in vivo)
Several animal models have been investigated for the identification of respiratory sensitizers, many of which were adapted from established skin sensitization methods. However, none of these approaches has been validated for regulatory use as a respiratory sensitization test.
Example of these animal-based approaches:
- Respiratory LLNA: Modified Local Lymph Node Assay.
- Mouse, rat, and guinea pig sensitization models.
- Inhalation toxicity studies (OECD TG 403, 412, 413).
Limitations:
- Lack of specificity for respiratory sensitization.
- Inability to reliably distinguish sensitization vs irritation.
- Limited relevance to human disease mechanisms.
- Increasing ethical and regulatory restrictions.
New Approach Methodologies (NAMs)
To address these limitations and support the transition away from animal testing, significant efforts are being directed toward NAM development within IATA frameworks.
Most NAMs are designed to address specific mechanistic elements of the respiratory sensitization AOP, although the relationships between assay endpoints and individual Key Events (KEs) are not yet fully validated or standardized. (Figure 5.1, OECD DRP, 2025).
Among the emerging non-animal approaches, GARD®air represents one of the most well-characterized and commercially available assays. It is supported by published data demonstrating high specificity and broad applicability across diverse chemical classes.
In silico/computational approaches
Examples: OECD QSAR Toolbox, CADRE, Toxtree, COEH
- Identify structural alerts and predict chemical reactivity with cell proteins, addressing the MIE/KE1.
- Useful for screening and prioritization.
- Cannot distinguish respiratory vs skin sensitizers.
- Limited ability to predict in vivo dosimetry and exposure context.
In chemico methods
Examples: DPRA, ADRA (OECD 442C for skin sensitization)
- Measuring protein reactivity, addressing the MIE/KE1.
- Validated only for skin sensitization.
- Do not account for metabolic activation (pro-haptens).
- Cannot differentiate respiratory vs skin sensitization.
In vitro methods
GARD®air
- Measures 28 genetic biomarkers associated with KE2-KE3.
- Uses a human dendritic-like cell line (SenzaCell®).
- Integrates genomics and machine learning for prediction.
- Demonstrated high specificity and broad applicability across diverse substances.
- Commercially available.
- Currently under evaluation in larger datasets and regulatory contexts.
AliSens
- Air–liquid interface model incorporating multiple lung cell types.
- Measures biomarkers associated with KE2–KE3.
- Commercially available.
- Limited datasets and validation across broader chemical domains.
Modified h-CLAT, DCsens, DC/Tsens
- Co-culture systems combining epithelial cells, dendritic cells, and/or T cells.
- Designed to investigate immune activation and intercellular signalling across KE2–KE4.
- Aim to capture biological processes such as dendritic cell maturation and T-cell polarization.
- May provide improved biological relevance compared to single-cell assays.
- Still under development and not standardized.
- Limited datasets and validation across broader chemical domains.
- Ability to consistently distinguish respiratory vs skin sensitizers remains under evaluation.
In vitro alveolar model
- 3D respiratory models used for transcriptomic profiling.
- Show potential to differentiate sensitizers vs non-sensitizers.
- Limited validation and chemical diversity.
- Further studies needed to identify critical pathways inducing respiratory sensitisation.
Ex vivo approaches
Precision-cut lung slices (PCLS)
- Preserve native lung architecture and cell composition.
- High physiological relevance.
- Not suitable for high-throughput screening.
- Primarily used for mechanistic research rather than routine hazard identification.
Current challenges in the field
Respiratory sensitization testing remains one of the most complex endpoints in toxicology due to a combination of scientific, methodological, and regulatory challenges, many of which are directly linked to the underlying biology of the endpoint.
Unique technical challenges
Several challenges are intrinsic to respiratory sensitization and fundamentally limit the development of predictive test methods:
Irritant vs. sensitizer discrimination
Discriminating between a true immunological respiratory sensitizer and a non-immunological chemical irritant remains a central challenge. Both can induce airway inflammation and respiratory symptoms, making mechanistic differentiation difficult in both in vitro and in vivo systems.
Exposure and delivery systems
Accurately replicating the physiology of the human respiratory tract in vitro requires controlled exposure systems, such as air–liquid interface models. These systems are technically demanding to design, standardize, and reproduce, particularly for volatile or poorly soluble substances.
Systemic and multi-step biology
Respiratory sensitization is a systemic, multi-stage process involving coordinated responses across multiple cell types and tissues. No single in vitro model can capture the full sequence from induction to elicitation. As a result, assessment depends on integrated approaches, combining multiple assays within a weight-of-evidence (WoE) or IATA framework.
Other challenges
In addition to these core technical constraints, several broader challenges further complicate assessment:
Mechanistic complexity
- Involvement of multiple immune pathways.
- Differences in mechanisms across chemical classes and sensitizer types.
Methodological limitations
- Lack of validated, regulatory-accepted test methods.
- Limited ability of current models to fully represent the AOP.
- Technical difficulty in testing inhalable or reactive substances.
Data gaps
- Limited availability of large, high-quality datasets.
- Absence of standardized potency metrics and classification thresholds.
Exposure variability
- Multiple exposure routes (inhalation and dermal).
- Significant inter-individual variability (e.g., genetics, health status, co-exposures).
Conclusion
Respiratory sensitization is a scientifically evolving and regulatorily challenging endpoint with significant implications for occupational and public health.
Progress depends on:
- Improved mechanistic understanding
- Development of validated human-relevant NAMs
- Integration of experimental, computational, and clinical data
Adopting a mechanistically informed and integrated testing strategy is essential for regulatory compliance, proactive risk management, and safer product development.
Respiratory sensitization assessment is gradually transitioning from reliance on imperfect surrogate methods toward a more predictive, mechanism-driven discipline. Leveraging AOP frameworks and integrating in silico, in chemico, and in vitro NAMs enables earlier and more reliable hazard identification, providing a clear advantage in both product safety and regulatory readiness.
However, these approaches are still under development and require further validation before full regulatory acceptance can be achieved.
Discuss Your Respiratory Sensitization Challenges with Our Experts
Supported by industry collaborations and case studies, GARD®air has demonstrated robust performance across diverse substance categories, including industrial chemicals, proteins, and microorganisms.
Connect with our scientific experts to explore the scientific data and learn how the assay can support your respiratory sensitization assessment strategy.

About the Author

Andy Forreryd, PhD
In vitro toxicology expert, member of the OECD expert group on respiratory sensitization, member of ISO/TC 194/WG 8
Dr Andy Forreryd is an in vitro toxicology expert with extensive experience in assay development, genomics, and machine learning. He collaborates closely with industry leaders to advance novel applications of New Approach Methodologies (NAMs) for sensitization testing, with the aim to replace animal studies.
Dr Forreryd is a co-developer of the GARDskin assay (OECD TG 442E) for the assessment of chemical sensitizers. He is an active member of the OECD expert group on respiratory sensitization, and ISO/TC 194/WG 8 for skin sensitization testing of medical devices.
References
- OECD Detailed Review Paper (DRP) to facilitate the Development of Test Methods to Predict the Respiratory Sensitisation Potential of Low Molecular Weight Chemicals (2025): For public consultation
- OECD Test Guidline No. 442C (2026): In Chemico Skin Sensitisation
- OECD Test Guidline No. 442D (2026): In Vitro Skin Sensitisation
- OECD Test Guidline 442E (2024): In Vitro Skin Sensitisation
